
Welcome from Jan K. Carney, M.D., M.P.H.
Welcome to the Larner College of Medicine Graduate Public Health Program! Our mission is to prepare skilled and versatile graduates who lead through research, education, and practice. We invite you to join us in shaping a healthier future for all.
Director's Welcome Message
Become a Doctor of Public Health
Our new online DrPH program begins enrollment this Fall!



Meet MPH Student Samantha Collins
Public Health & You
- 1791 university founded
- R1 Top Tier Research University (Carnegie classification)
- 459 acres main campus

Advancing Health Through Education
Explore our 100% online, CEPH-accredited Public Health Programs.
MPH Program OverviewAdvancing Health Through Education
Explore our 100% online, CEPH-accredited Public Health Programs.
MPH Program OverviewLarner College News
Larner Faculty to Lead Largest U.S. Medical Specialty Organization

Public Health Student Award Winners Announced

Strengthening Rural Health Care: Incentive Scholarships Help Medical Grads Put Down Roots in Vermont

WVNY-TV Notes Payne Testimony on Primary Care
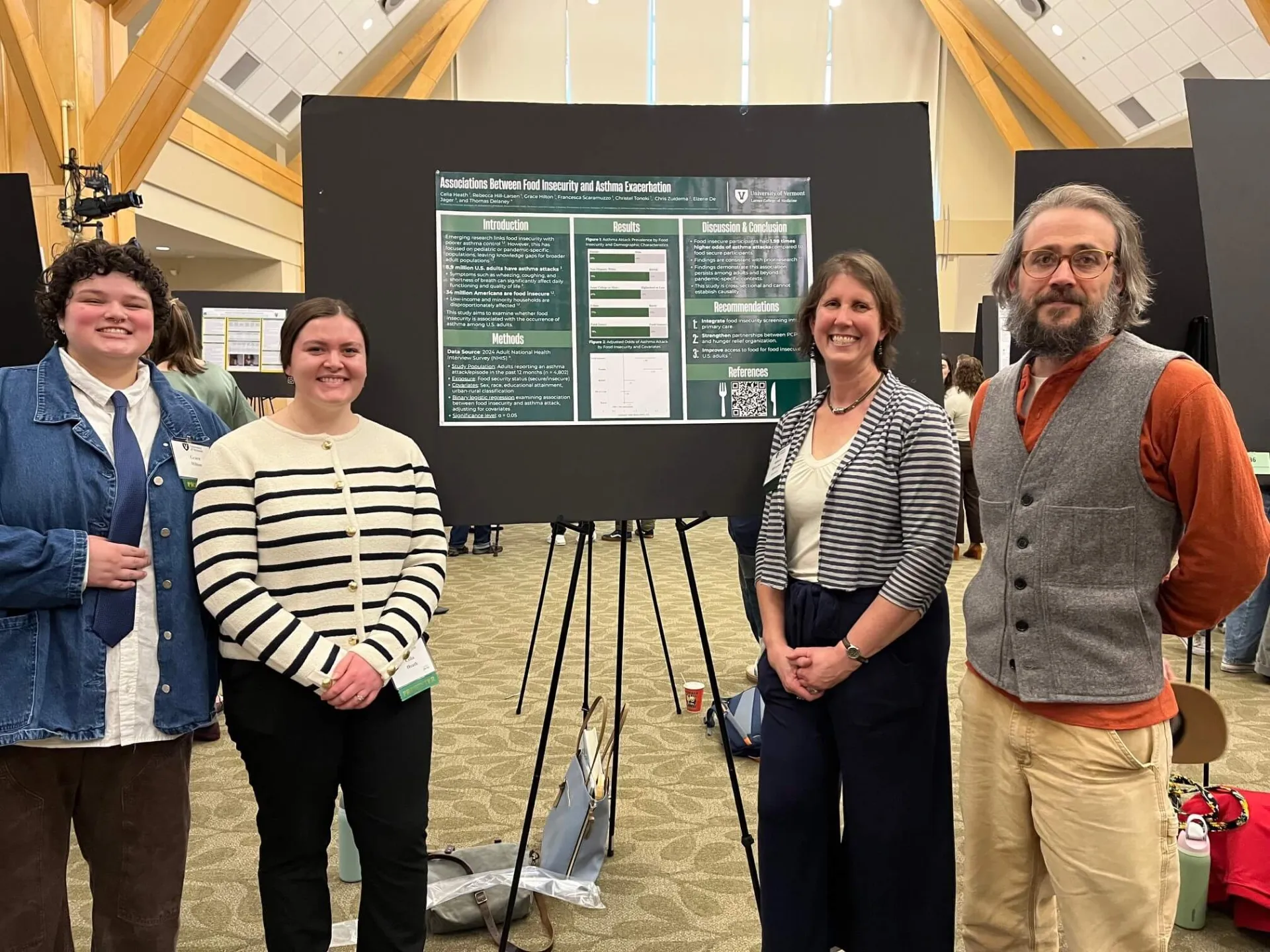
Public Health in Practice: MPH Students Present Culminating Research at 2026 UVM Student Research Poster Session.
Unparalleled Teaching and Expertise
Through groundbreaking research and hands-on fieldwork, our UVM Larner College of Medicine instructors bring unparalleled expertise to the classroom and learning environment.